
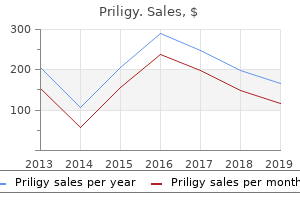
"Buy generic priligy on line, erectile dysfunction treatment costs".
By: J. Javier, M.B.A., M.B.B.S., M.H.S.
Professor, Marist College
It has a rapid onset of action and a lower risk of hypoglycemia than the sulfonylureas erectile dysfunction and diabetes type 1 order priligy with american express, and achieves better post-prandial glucose profiles impotence at 18 cheap priligy on line. Repaglinide is predominantly metabolized in the liver to inactive metabolites and is safe in mild to moderate renal impairment erectile dysfunction treatment san francisco buy priligy master card. Tablets can be missed if meals are omitted erectile dysfunction gel treatment buy priligy from india, and it may be effectively combined with metformin and with thiazolidinediones (where license permits). Nateglinide is a recent meglitinide which has a faster and shorter duration of insulin secretory activity than repaglinide but is less effective as monotherapy or in combination than rapaglinide. Insulin Recent improvements in the organization of care between hospital and primary care, and the expanding roles of diabetes specialist nurses and general practice nurses, have made it easier and safer to use insulin in the treatment of older people with diabetes [112]. Reported benefits include improvements in well-being and possibly quality of life [113115] and in cognitive function [70], partly following improved glycemic control; however, others have found lower treatment satisfaction in insulin-treated patients [116]. Rapidly acting insulin analogs such as insulin lispro or insulin aspart may cause less hypoglycemia and weight gain, and can be given after eating where timing may be Table 54. Once-daily insulin regimens alone are now little used, except where glycemic control is not a priority or injections are impracticable. Insulin can usefully be combined with an oral agent in patients failing to be controlled by diet and oral agents. For frail subjects including those within care-home settings, complex regimens should be avoided so the use of longer-acting insulin analogs during the day often combined with oral agents is a feasible alternative. Low-vision aids are available to help to inject insulin, and some insulin pens have audible clicks for counting doses. Screen on admission for diabetes and regularly thereafter Policies must include strategies to minimize hospital admission, metabolic decompensation, pressure-sore development, pain, diabetes-related complications, infections and weight loss All residents with diabetes must have an annual review and access to specialist services Care-home diabetes policies must be developed nationally, locally and at the level of the resident with diabetes Research based on interventional strategies is needed mologists, and poor knowledge and training for care staff [120,121]. The impact of these initiatives is being followed on outcomes including well-being, metabolic control, access to regular review, rates of hospitalization and diabetic complications such as amputation and visual loss. Modern diabetes care for older people Diabetic patients in care homes In many developed countries the numbers of care-home residents are increasing and the prevalence of diabetes in this setting will inevitably increase. People with diabetes in care homes should receive care commensurate with their health and social needs [121]. The best possible quality of life and well-being should be maintained, without unnecessary or inappropriate interventions, while helping residents to manage their own diabetes wherever feasible and worthwhile. Metabolic control should reduce both hyperglycemic lethargy and hypoglycemia, with a well-balanced dietetic plan that prevents weight loss and maintains nutritional well-being. Foot care and vision require screening and preventive measures to maintain mobility and prevent falls and unnecessary hospital admissions. At present, residents with diabetes in care homes appear to be generally vulnerable and neglected, with high prevalences of macrovascular complications and infections (especially skin and urinary tract), frequent hospitalization and much physical and cognitive disability. This emphasizes the importance of early intervention in diabetic complications and of establishing rehabilitation programs for patients disabled by various complications such as amputation, peripheral neuropathy, immobility, falls, stroke and cognitive change. Health care must be cost-effective, which presents a difficult challenge for diabetes, because of its high prevalence, long duration of impact and wide spectrum of complications and emotional and psychologic sequelae; in older subjects, the challenge is even more complex because of the many other confounding factors. Hospital admissions of diabetic patients: information from hospital activity analysis. Improving the care of elderly diabetic patients: the final report of the St Vincent Joint Task Force for Diabetes. Some observations on sugar tolerance with special reference to variations found at different ages. Fast-track vascular work-up with early surgical referral Expected benefits Early detection/ management of vascular complications Optimized functional status Improved quality of life and well-being Functional assessment/active screening for complications programme Aggressive treatment of blood pressure and dyslipidemia Critical event monitoring Aggressive glucose control in acute myocardial infarction and stroke Developing rehabilitation programmes Figure 54. Recent studies [127129] have suggested that aggressive treatment of diabetes in older individuals is not warranted because of their reduced life expectancy; however, implementing the strategies outlined above seems likely to reduce acute hospitalization, outpatient costs and long-term disability. Only well-organized prospective clinical trials will be able to determine how best to manage diabetes in older people. Ambulatory medical care for elderly diabetics: the Fredericia survey of diabetic and fasting hyperglycemic subjects aged 6074 years. Use of hospital services by elderly diabetics: the Frederica Study of diabetic and fasting hyperglycemic patients aged 6074 years.
More frequent antenatal visits while not necessarily Management of Second Trimester Loss Second trimester loss deserves the same emotional care and support outlined above erectile dysfunction pills cost priligy 60 mg mastercard. Clinical management following diagnosis includes offering the option of labor induction or dilatation and evacuation (D&E) erectile dysfunction doctors los angeles buy priligy with amex. Maternal grief resolution is not affected by the choice of termination if the woman self-selects the process erectile dysfunction protocol pdf cheap priligy 60 mg with amex. From 13 to 17 weeks use 200 mcg every 6 to 12 hours with the potential to double the dose to 400 mcg q 6 to 12 hours if the first dose does not result in adequate contractions impotence 20 years old priligy 60 mg sale. For 18 to 26 weeks start with 100 mcg q 6 to 12 hours and consider doubling to 200 mcg q 6 to 12 hours if the first dose does not provide adequate contractions. In women with a prior uterine scar consider a lower initial dose and do not double after the first dose is given. Without "full disclosure" and transparency, parents are hardly prepared to make an informed choice as to whether to test or 6 Chapter R - Birth Crisis not. Before proceeding with testing parents need to be carefully counseled as to the limits of testing and the potential choices they may face. The same emotional support and counseling should be made available to parents who choose to terminate a pregnancy as to those who experience the spontaneous loss of a baby. The maternal mortality rate in the United States appears to no longer be decreasing, perhaps due to the obesity epidemic and the increased proportion of births that are by cesarean. However, across Australia more than one woman dies every two weeks in circumstances associated with childbearing. The Baby with an Abnormality or Disability Caring for a child with disabilities is a stressful situation for the parents, and the best predictor of the level of stress is the severity of the disability. There is some evidence that family centered care provides the best support for caregivers of children with disabilities. Parents should be offered information about community resources available for the particular condition and directed to any support groups that are available. Maternal Critical Illness and Death While this chapter concentrates on the experience of birth crisis in relation to the baby, the death of or critical illness of a mother in pregnancy or around childbirth is equally important and distressing for all. Maternal critical illness may be related to prior comorbidities such as obesity or hypertension. It may also occur as a result of a pregnancy complication such as preeclampsia or hemorrhage. Prenatal recognition of a high-risk pregnancy is important in ensuring the appropriate level of care is offered with the utilization of and referral to the maternal fetal medicine team as appropriate. All facilities providing obstetric care must be prepared to handle emergencies such as massive blood loss, maternal seizure and sepsis. The implementation of evidence-based protocols will help guide providers in facilities without immediate access to an intensive care team. The amount of support that providers need to deal with their own grief or fears should not be under-estimated. One common theme from these studies is that staff often experience guilt as they feel that their role is about saving lives rather than being around death. Self-doubt, self-blame and depression were also frequent reactions experienced by the physician. In these environments, there is often little time to grieve, acknowledge the event, and assess how they might be impacted by them. These include reflection and review; emotional and practical support; access to counselling services; initial and ongoing education and training; institutional policies and guidelines. Peer support groups, multidisciplinary team meetings and formal debriefing with trained personnel are all strategies that can provide support for clinicians. An element of personal healing needs to take place to enable health care providers to move beyond the strong emotions after a perinatal loss. Formal reflection on the care of the woman during her pregnancy with colleagues is also very important.
Since uE3 has been shown to be more accurate than clinical assessment in predicting labor onset erectile dysfunction drugs online order 60mg priligy visa, there is increasing interest in its use in assessment of pre-term labor risk erectile dysfunction 38 years old discount 30 mg priligy overnight delivery. High maternal serum uE3 levels may also be occasionally observed in various forms of congenital adrenal hyperplasia psychological reasons for erectile dysfunction causes discount priligy 30mg with amex. An elevated serum or uE3 above 3 multiples of the gestational age mean youth erectile dysfunction treatment buy 30mg priligy, or with an absolute value of more than 2. In the context of assessment of a patient deemed at risk of preterm labor, a single serum or uE3 measurement within the above cutoffs, has a negative predictive value of labor onset (ie, labor unlikely within the next 4 weeks) of 98% in low-risk populations and of 96% in high-risk populations. Measurements of serum uE3 performed in the context of epidemiological or other basic or clinical scientific studies need to be interpreted in the context of those studies. Useful For: the test is most frequently used in breast carcinomas when decisions on hormonal therapy must be made. While the test can be performed on any formalin-fixed, paraffin-embedded tissue, it is infrequently used for non-breast cancer specimens. Interpretation: Immunoperoxidase-stained slides are examined microscopically by the consulting anatomic pathologist and interpreted as negative (<1% reactive cells), focally positive (1%-10% reactive cells), or positive (>10% reactive cells). Ogawa Y, Moriya T, Kato Y, et al: Immunohistochemical assessment for estrogen receptor and progesterone receptor status in breast cancer: analysis for a cutoff point as the predictor for endocrine therapy. They also are important for many other, non-gender-specific processes, including growth, nervous system maturation, bone metabolism/remodeling, and endothelial responsiveness. The 2 major biologically active estrogens in nonpregnant humans are estrone (E1) and estradiol (E2). E2 and E1 can be converted into each other, and both can be inactivated via hydroxylation and conjugation. E2 levels then rise gradually until 2 to 3 days before ovulation, at which stage they start to increase much more rapidly and peak just before the ovulation-inducing lutenizing hormone/follicle stimulating hormone surge at 5 to 10 times the early follicular levels. E2 levels then gradually increase again until the midpoint of the luteal phase and thereafter decline to trough, early follicular levels. Measurement of serum E2 forms an integral part of the assessment of reproductive function in females, including assessment of infertility, oligo-amenorrhea, and menopausal status. In addition, it is widely used for monitoring ovulation induction, as well as during preparation for in vitro fertilization. However, extra sensitive E2 assays, simultaneous measurement of E1, or both are needed in a number of other clinical situations. These include inborn errors of sex steroid metabolism, disorders of puberty, estrogen deficiency in men, fracture risk assessment in menopausal women, and increasingly, therapeutic drug monitoring, either in the context of low-dose female hormone replacement therapy or antiestrogen treatment. Useful For: this test allows the simultaneous high-sensitivity determination of serum estrone and estradiol levels. It is useful in situations requiring either higher sensitivity estradiol measurement, or estrone measurement, or both. This includes the following: -As part of the diagnosis and work-up of precocious and delayed puberty in females, and, to a lesser degree, males -As part of the diagnosis and work-up of suspected disorders of sex steroid metabolism, eg, aromatase deficiency and 17 alpha-hydroxylase deficiency -As an adjunct to clinical assessment, imaging studies, and bone mineral density measurement in the fracture risk assessment of postmenopausal women, and, to a lesser degree, older men -Monitoring low-dose female hormone replacement therapy in postmenopausal women -Monitoring antiestrogen therapy (eg, aromatase inhibitor therapy) Useful in all applications that require moderately sensitive measurement of estradiol including: -Evaluation of hypogonadism and oligo-amenorrhea in females -Assessing ovarian status, including follicle development, for assisted reproduction protocols (eg, in vitro fertilization) In conjunction with luteinizing hormone measurements, monitoring of estrogen replacement therapy in hypogonadal premenopausal women Evaluation of feminization, including gynecomastia, in males Diagnosis of estrogen-producing neoplasms in males, and, to a lesser degree, females Interpretation: Estradiol (E2) levels below the premenopausal reference range in young females indicate hypogonadism. This can have functional causes, such as starvation, overexercise, severe physical or emotional stress, and heavy drug and/or alcohol use. Irregular or absent menstrual periods with normal or high E2 levels (and often high estrone [E1] levels) are indicative of possible polycystic ovarian syndrome, androgen producing tumors, or estrogen producing tumors. E2 analysis may be helpful in establishing time of ovulation and optimal time for conception. Optimal time for conception is within 48 to 72 hours following the midcycle E2 peak. Serial specimens must be drawn over several days to evaluate baseline and peak total estrogen (E1 + E2) levels. Low baseline levels and a lack of rise, as well as persistent high levels without midcycle rise are indicative of anovulatory cycles. For determining the timing of initiation of ovarian stimulation in in vitro fertilization studies, low levels (around 30 pg/mL) before stimulation are critical, as higher values often are associated with poor stimulation cycles. Estrogen replacement in reproductive age women should aim to mimic natural estrogen levels as closely as possible.
Hyperviscosity may be manifested by oronasal bleeding drugs for erectile dysfunction pills buy cheap priligy on-line, blurred vision erectile dysfunction medication otc generic priligy 30 mg with amex, headaches erectile dysfunction juice recipe cost of priligy, dizziness erectile dysfunction drugs herbal purchase priligy 90 mg on-line, nystagmus, deafness, diplopia, ataxia, paresthesias, or congestive heart failure. Funduscopic examination reveals dilation of retinal veins and flame shaped retinal hemorrhages. Because the ability of a monoclonal protein to cause hyperviscosity is affected by its concentration, molecular weight, and aggregation, sera with concentrations of monoclonal IgM >4 g/dL, IgA >5 g/dL, or IgG >6 g/dL should be tested for hyperviscosity. Serum viscosity and electrophoresis are recommended before and after plasmapheresis in order to correlate viscosity and M-spike with patient symptoms. This correlation may be useful for anticipating the need for repeat plasmapheresis. Useful For: Detection of increased viscosity Monitoring patients with hyperviscosity syndrome Interpretation: Although viscosities >1. Together with certain carotenoids, vitamin A enhances immune function, reducing the consequences of some infectious diseases. Poor adaptation of vision to darkness (night blindness) is an early symptom that may be followed by degenerative changes in the retina. In developing countries, vitamin A deficiency is the principal preventable cause of blindness. In particular, chronic vitamin A intoxication is a concern in normal adults who ingest >15 mg per day, and in children who ingest >6 mg per day of vitamin A over a period of several months. Liver fibrosis with portal hypertension and bone demineralization may also result. Vitamin E: Vitamin E contributes to the normal maintenance of biomembranes, the vascular system, and the nervous systems; and provides antioxidant protection for vitamin A. Currently, the understanding of the specific actions of vitamin E is very incomplete. The tocopherols (vitamin E and related fat-soluble compounds) function as antioxidants and free-radical scavengers, protecting the integrity of unsaturated lipids in the biomembranes of all cells and preserving retinol from oxidative destruction. Those influences on thrombocyte aggregation may be of significance in relation to risks for coronary atherosclerosis and thrombosis. Premature infants who require an oxygen-enriched atmosphere are at increased risk for bronchopulmonary dysplasia and retrolental fibroplasia. Supplementation with vitamin E has been shown to lessen the severity of, and may even prevent, those problems. In addition, low blood levels of vitamin E may be associated with abetalipoproteinemia, presumably as a result of a lack of the ability to form very low-density lipoproteins and chylomicrons in the intestinal absorptive cells of affected persons. Chronically excessive ingestion has been suspected as a cause of thrombophlebitis, although this has not been definitively verified. Deficiencies of vitamins A and E may arise from poor nutrition or from intestinal malabsorption. Persons, especially children, at risk include those with bowel disease, pancreatic disease, chronic cholestasis, celiac disease, cystic fibrosis, and intestinal lymphangiectasia. Infantile cholangiopathies that may lead to malabsorption of vitamins A and E include intrahepatic dysplasia and rubella-related embryopathy. Useful For: Diagnosing vitamin A deficiency and toxicity Evaluating persons with intestinal malabsorption of lipids Evaluating individuals with motor and sensory neuropathies for vitamin E deficiency Monitoring vitamin E status of premature infants requiring oxygenation Interpretation: Vitamin A: the World Health Organization recommendations supplementation when vitamin A levels fall below 20. Vitamin E (alpha-tocopherol): -Values that indicate need for supplementation: -Premature: <2. Vitamin A plays an essential role in the function of the retina (adaptation to dim light), is necessary for growth and differentiation of epithelial tissue, and is required for growth of bone, reproduction, and embryonic development. Degenerative changes in eyes and skin are commonly observed in vitamin A deficiency. Severe or prolonged deficiency leads to dry eye (xerophthalmia) that can result in corneal ulcers, scarring, and blindness. Another important consequence of inadequate intake is acquired immunodeficiency disease, where an increased incidence of death is associated with deficient vitamin A levels. In particular, chronic vitamin A intoxication is a concern in normal adults who ingest >15 mg per day and children who ingest >6 mg per day of vitamin A over a period of several months. Manifestations are various and include dry skin, cheilosis, glossitis, vomiting, alopecia, bone demineralization and pain, hypercalcemia, lymph node enlargement, hyperlipidemia, amenorrhea, and features of pseudotumor cerebri with increased intracranial pressure and papilledema. Congenital malformations, like spontaneous abortions, craniofacial abnormalities, and valvular heart disease have been described in pregnant women taking vitamin A in excess. Useful For: Diagnosing vitamin A deficiency and toxicity Monitoring vitamin A therapy Interpretation: the World Health Organization recommendations supplementation when vitamin A levels fall below 20.
An ionophore is a compound that is capable of selectively carrying ions across a membrane erectile dysfunction 40s order generic priligy online. The ion fits into a specific binding site in a molecule that is hydrophobic enough to cross the membrane impotence grounds for annulment discount 60 mg priligy with amex. Electrochemical gradient is the name given to the gradient of charge and ions that exists across the inside and the outside of a cellular membrane erectile dysfunction options buy cheap priligy 30mg. The outside of the mitochondrion is more positively charged than the inside most effective erectile dysfunction drugs buy discount priligy 60mg, and the concentration of potassium ions is higher outside than inside. When an ion falls through (an expression that gives a nice image, but moves would be just as good) the electrochemical gradient, it is driven by both its concentration gradient and the charge difference between the inside and the outside of the membrane. The bigger the charge difference between the inside and the outside, the bigger the free-energy difference that drives the ion movement (see Chapter 3). Cyanide blocks the last step of electron transfer by combining with and inhibiting cytochrome oxidase. The less obvious effect is that all the electron carriers become more reduced than they would be without the inhibitor. The reason is that the substrates are still pushing reducing equivalents (electrons) down the electron transport chain. The general rule is that all electron carriers that occur before the block become reduced and all that occur after the block become oxidized. All intermediates before and including cyt a will be in the reduced state; all intermediates after and including cyt c1 will be in the oxidized state. The -glutamyl part means that the amino group of the cysteine is attached to the side chain carboxyl group of the glutamic acid rather than to the -carboxyl. Notice that some of the amino acids require other amino acids for their synthesis. Exam questions usually center on whether or not an amino acid is essential and the metabolites that serve as precursors for specific amino acids. The complete catabolic pathways of the individual amino acids are a complex set of pathways that are probably not worth remembering in detail (this is obviously opinion). In fact, there are diseases that are caused by inherited defects in most of the pathways. The preceding table is a general guide that shows where the amino acids go and points out significant intermediates. Nitrogen is dumped into the urea cycle by transamination to make Asp or Glu or by deamination to make ammonia. One of the early, if not the first, steps in amino acid catabolism involves a transamination using oxaloacetate or ketoglutarate as the amino-group acceptor. This converts the amino acid into a 2-keto acid, which can then be metabolized further. In addition, pyridoxal phosphate is also required for most decarboxylations, racemizations, or elimination reactions in which an amino acid is a substrate. Pyridoxal phosphate is not involved in decarboxylations in which the substrate is not an amino acid. So if a question 16 Amino Acid Metabolism · 189 · asks something about an amino acid and a vitamin, the answer will most likely be pyridoxal phosphate. There are a couple of exceptions in which pyridoxal phosphate may not be the answer to a vitamins-amino acid question. If the amino acid is serine, then the answer might also include folic acid (the reaction here is the conversion of serine to glycine with the formation of methylene tetrahydrofolic acidsee the section in Chap. The other place you might see a vitamin other than pyridoxal phosphate is in the metabolism of propionyl-CoA, a product of the catabolism of some amino acids. In this case, the vitamin may be B12 (the conversion of methylmalonyl-CoA to succinylCoA-see " -Oxidation Odd-Chain-Fatty Acids" in Chap. The nitrogen from the amino groups of most amino acids is transaminated into glutamate or aspartate at some point in the degradative scheme. This nitrogen enters the urea cycle as glutamate, which is reductively deaminated by glutamate dehydrogenase to yield ammonia or by the reaction of aspartate with citrulline to give argininosuccinate (urea cycle). As you prowl around the individual metabolic pathways of energy metabolism, you need to get a feel for the kinds of things you should be looking for as you examine each metabolic scheme. Next, understand when the pathway should be on or off-what metabolic states require the pathway to function.
Buy 30 mg priligy visa. How To Cure Erectile Dysfunction Naturally And Permanently.