
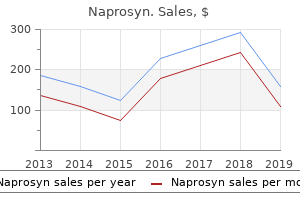
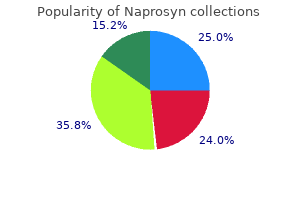
"Naprosyn 500 mg sale, rheumatoid arthritis z deformity".
By: P. Hjalte, MD
Clinical Director, Southern Illinois University School of Medicine
Since blood from the lungs flows directly to the brain arthritis in neck can it cause dizziness naprosyn 500 mg low cost, lung cancer is capable of quickly spreading to the brain rheumatoid arthritis leg pain purchase naprosyn toronto. Sometimes arthritis guitar 250mg naprosyn with visa, this happens so fast that the brain metastases are found before the primary lung cancer is found rheumatoid arthritis labs buy generic naprosyn 500mg. Scientists also know that primary cancers tend to send cells to particular organs. It is believed these organ preferences may be caused by small attractant molecules, chemokines, that direct and guide tumor cells to the metastatic site. In other instances cancer cells may be able to adhere, or stick, only to select organs based upon adherent molecules expressed in a particular organ. While swelling around the tumor is more common, bleeding from ruptured blood vessels in the tumor occurs in a small percentage of patients. Headaches may also be caused by cystic (water filled cavities) changes in the tumor or by interruption of spinal fluid circulation in brain resulting in a condition called hydrocephalus. During normal electrical activity, the nerve cells in the brain communicate with each other through carefully controlled electric signals. During a seizure, abnormal electrical activity occurs, that may stay in a small area or spread to other areas of brain. Disturbance in the way one thinks and processes thoughts (cognition) is another common symptom of a metastatic brain tumor. Cognitive challenges might include difficulty with memory (especially short term memory) or personality and behavior changes. Motor problems, such as weakness on one side of the body or an unbalanced walk, can be related to a tumor located in the part of the brain that controls these functions. Metastatic tumors in the spine may cause back pain, weakness or changes in sensation in an arm or leg, or loss of bladder/bowel control. Both cognitive and motor problems may also be caused by edema, or swelling, around the tumor. Metastatic tumors are diagnosed using a combination of neurological examination and imaging (also called scanning) techniques. The images will help your physician learn: · Size and number of tumors · Exact location of the tumor(s) within the brain or spine · Impact on nearby structures Although scans provide the physician with a "probable" diagnosis, examination of a sample of tumor tissue under a microscope confirms the exact pathologic diagnosis. The tissue sample may be obtained during surgery to remove the tumor, or during a biopsy. If a metastatic tumor is diagnosed before the primary cancer site is found, tests to locate the primary site will follow. The neurosurgeon will look at your scans to determine if the tumor(s) can be surgically removed, or if other treatment options would be more reasonable for you. When planning your treatment, your doctor will take several factors into consideration. Reducing the swelling in the brain can reduce the raised brain pressure, and thus temporarily reduce the symptoms of a metastatic brain tumor. Research shows that the number of metastases is not the sole predictor of how well you might do following treatment. Your neurological function (how you are affected by your brain metastases) and the status of the primary cancer site. Treatment decisions will take into account not only long term survival possibilities, but your quality of life during and after treatment, as well as cognition concerns. That radiation may be whole-brain radiation therapy, whole-brain radiation plus stereotactic radiosurgery or stereotactic radiosurgery alone. This is generally followed by medical therapy (chemotherapy, radiation therapy or immune-based therapy) that may impact not only the primary cancer but also metastatic brain tumor. However in more recent times there is an increase in the use of radiosurgery or medical therapy (chemotherapy, targeted therapy or immune-based therapy) for these patients. If there is a question about the scan results or the diagnosis, a biopsy or surgery to remove the brain tumors may be done. This will allow your physicians to confirm that the brain tumors are related to your cancer. If you do not have a history of cancer, your physicians will order tests to try to determine the primary site. If no other cancer site is found, surgery to obtain a tissue sample may be performed. In general, the primary treatment for multiple metastatic brain tumors (or multiple tumors that are not close to each other) is whole-brain radiation.
It follows that school athletic programs must reflect the value of equal opportunity in all policies and practices arthritis of feet diagnosing discount naprosyn online. Athletic programs affiliated with educational institutions have a responsibility treatment for arthritis in feet and ankles discount naprosyn uk, beyond those of adult amateur or professional sports programs arthritis suitable diet order naprosyn 500mg, to look beyond the value of competition to promote broader educational goals of participation arthritis pain management uk discount 500 mg naprosyn with amex, inclusion, and equal opportunity. Because high schools and colleges must be committed to those broader educational goals, they should not unthinkingly adopt policies developed for adult Olympic and professional athletes. Recognizing the need to address the participation of transgender athletes, a few leading international and professional sport governing organizations have developed policies based on overly stringent, invasive, and rigid medical requirements. These policies are not workable or advisable for high school and college athletes for a number of reasons. Lisa mottet, National Gay and Lesbian Task Force Policy Institute and National Center for Transgender Equality, "Preliminary Findings of the National Transgender Discrimination Survey" (2010). High school- and college-aged student athletes have developmental needs that differ from those of adults. For example, a core purpose of high school and college is to teach students how to participate and be good citizens in an increasingly diverse society and how to interact respectfully with others. In addition, high school and college athletic programs impose limits on how many years a student athlete can compete that do not exist in adult sporting competitions, where athletes can compete as long as their performances are viable or, in the case of most amateur sports, as long as they wish to . It is also advisable that high school athletic programs adopt a different policy for including transgender student athletes than college athletic programs. In contrast, the report recommends a more nuanced policy for collegiate athletics that is based, in part, upon whether a student athlete is undergoing hormone therapy. The need for distinct high school and collegiate policies is based on several considerations. First, in high school settings, students are guaranteed the availability of a high school education and a corresponding opportunity to participate equally in all high school programs and activities. At the high school level, the focus should be on full participation in athletics for all students, within the limits of school resources to provide participation opportunities. Intercollegiate athletics are regulated nationally by governing bodies that sponsor national competitions and oversee such functions as the random testing of student athletes for the use of banned substances thought to enhance athletic performance. Because testosterone is a banned substance under the current rules for intercollegiate competition, the inclusion of transgender student athletes in college sports must be consistent with those rules. Third, high school student athletes are still growing and developing physically, cognitively, and emotionally. Because high school-aged students are still growing and maturing, they present a broader range of physical characteristics than collegiate student athletes do, and these differences should be taken into account in developing a policy for high school students. Finally, high school-aged and younger transgender students are subject to different medical protocols than adults because of their age and physical and psychological development. Those protocols vary based on the age and psychological readiness of the young person. For youth who are approaching puberty, hormone blockers may be prescribed to delay puberty in order to prevent the youth from going through the traumatic experience of acquiring secondary sex characteristics that conflict with his or her core gender identity. For older youth, cross-gender hormones or even some sex-reassignment surgeries may be prescribed. In the high school and college policies recommended below, we have attempted to take account of these differences. Shou ld thePart i ci pat i onofTra n s g en d erSt u d en t At h le tes o n Sc h o o l Tea ms Rai seConcernsAboutCo m p et it iveE q u it y? Concern about creating an "unfair competitive advantage" on sex-separated teams is one of the most often cited reasons for resistance to the participation of transgender student athletes. These concerns are based on three assumptions: one, that transgender girls and women are not "real" girls or women and therefore not deserving of an equal competitive opportunity; two, that being born with a male body automatically gives a transgender girl or woman an unfair advantage when competing against non-transgender girls and women; and three, that boys or men might be tempted to pretend to be transgender in order to compete in competition with girls or women. For many transgender people, gender transition is a psychological and social necessity. Second, while some people fear that transgender women will have an unfair advantage over nontransgender women, it is important to place that fear in context.
Purchase 500mg naprosyn visa. The Diet that Cures Arthritis Joint Pain and Rheumatoid Arthritis in Just 120 Days?.
In addition arthritis in fingers relieve discount naprosyn online amex, the effects of oral hypoglycemics developed for the general population will need to be evaluated in this patient subgroup arthritis weight lifting safe naprosyn 250 mg. However rheumatoid arthritis factor range purchase naprosyn 500mg with visa, the best practice for following and managing patients is unknown and will need to be established by collaboration between various expert providers arthritis pain in feet and hands 500mg naprosyn otc. Further challenges in these areas will be provided by integrating the side-effects of prior and ongoing therapies with management of these, and other, results of normal aging. Transition of Care Transition of care from pediatric to adult medicine is an important issue in young adults with complex and chronic illnesses. European countries with comprehensive state-supported health care systems have often taken the lead in the development of these transition systems. In most centers, pediatric services define their target population by age, and adults may not be treated by pediatric subspecialists or in pediatric in-patient facilities. Young adult patients must develop independence and undertake personal responsibility for their health care. Timing of transition is important and must be seen as a process, not an abrupt transfer of services. Data show 270 Fanconi Anemia: Guidelines for Diagnosis and Management that the most successful transitions are initiated at a very early stage with prospective education of the family and patient regarding future transition. In contrast, timing may be very situation-dependent, as it is likely to be inappropriate to transition a patient with quickly progressing disease or at the "end of life. Focus groups and surveys have identified barriers to transition,4,7,8-11 including: · Reluctance of patients and their families to leave trusted health care providers and comfortable clinical settings. Differences in approaches to the chronically ill by pediatric and adult providers; i. Concerns about the experience, knowledge base and quality of care that will be offered by specialists in adult medicine in regard to childhoodonset diseases. As in all childhood diseases, surrogate decision-making imposes many demands on parents and guardians. There is a potential risk of parental over-protectiveness in the setting of requisite attention to safety, and the age-appropriate pursuit of adolescent independence may be particularly difficult for parents. Recent follow-up of adult survivors of childhood acute lymphoblastic leukemia shows more adverse mental health functional impairment and activity limitations compared with their healthy siblings. Studies to date show that these latter issues of adulthood are also inadequately addressed in many pediatric healthcare settings, thus further exacerbating the stress on patients and families. Medical compliance may also be an issue, particularly during adolescence and during the transition period. For individuals newly diagnosed in adulthood, the ramifications of established relationships (with spouses, partners, employers, etc. The knowledge base is as yet insufficient for understanding best practices, and the provider pool within the community of physicians caring for adult patients is not yet well educated as to either the nature of the disorder or the needs of the patients. Improving transition from pediatric to adult cystic fibrosis care: lessons from a national survey of current practices. Risk of head and neck squamous cell cancer and death in patients with Fanconi anemia who did and did not receive transplants. Strategies for improving transition to adult cystic fibrosis care, based on patient and parent views. Trends in transition from pediatric to adult health care services for young adults with chronic conditions. Transition programs in cystic fibrosis centers: perceptions of pediatric and adult program directors. Twenty-five-year follow-up among survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. Additionally, the consultation should include information about current research opportunities and support groups, future reproductive options and their familial implications. This history can be helpful in determining the inheritance pattern as well as the genetic basis of the disease.
Thyroxine made in a lab is exactly the same hormone that a human thyroid makes arthritis pain relief juice generic 250mg naprosyn with visa, but in a pure form arthritis in the back ribs discount naprosyn 500mg with visa. Once the thyroid stops functioning xanax arthritis pain naprosyn 500 mg with amex, taking extra iodine or other substances will not help it work better arthritis medication kidney discount naprosyn master card. If you take too much, you can develop the symptoms of hyperthyroidism-an overactive thyroid. The most common symptoms of too much thyroid hormone are fatigue, the inability to sleep, greater appetite, nervousness, shakiness, feeling hot when other people are cold, muscle weakness, shortness of breath, and a racing, skipping heart. Hyperthyroidism can also cause changes that you cannot feel, like bone loss (osteoporosis) and an irregular heartbeat. On the day of your blood test, you should take your thyroxine the same way and time that you always do - it does not need to be held for the blood test. For example, if a lab runs two tests on one blood sample, it may get two slightly different results. Rather than stopping your pills completely, you might ask your doctor to try lowering your dose. If a baby does not get enough thyroid hormones, it cannot maintain normal thyroid hormone levels before or after birth. People who live in parts of the world where they do not get enough iodine from their food may develop hypothyroidism. Worldwide, iodine deficiency is the major cause of hypothyroidism and preventable mental retardation. Subclinical (mild) hypothyroidism may never get worse or it may get worse over months or years. To survive a myxedema coma, people need good supportive care in the hospital intensive care unit. When you go for visits, you have to tell your doctor how you are feeling and be honest in saying how often you miss your pills. Before you visit your doctor, write a list of all the things you want to ask or tell her or him so you do not forget. It is important to be patient as you begin treatment-patient with yourself and the changes happening in your body, patient with your doctor, and patient with the people who are going through this with you. It can take weeks before the thyroxine begins to make you feel better and months before you and your doctor get the dose exactly right. The Complete Guide to the Causes, Symptoms, Diagnosis, and Treatments of Thyroid Problems (Foreword by George H. It occurs acutely in about 7% of patients who have limb fractures, limb surgery, or other injuries. Many cases resolve within the first year, with a smaller subset progressing to the chronic form. This transition is often paralleled by a change from "warm complex regional pain syndrome," with inflammatory characteristics dominant, to "cold complex regional pain syndrome" in which autonomic features dominate. Multiple peripheral and central mechanisms seem to be involved, the relative contributions of which may differ between individuals and over time. Possible contributors include peripheral and central sensitization, autonomic changes and sympatho-afferent coupling, inflammatory and immune alterations, brain changes, and genetic and psychological factors. Few high quality randomized controlled trials are available to support the efficacy of the most commonly used interventions. Reviews of available randomized trials suggest that physical and occupational therapy (including graded motor imagery and mirror therapy), bisphosphonates, calcitonin, subanesthetic intravenous ketamine, free radical scavengers, oral corticosteroids, and spinal cord stimulation may be effective treatments. Multidisciplinary clinical care, which centers around functionally focused therapies is recommended. Other interventions are used to facilitate engagement in functional therapies and to improve quality of life. In its most severe form, patients present with a limb displaying extreme hyperalgesia and allodynia (normally non-painful stimuli such as touch or cold are experienced as painful); obvious changes to skin color, skin temperature, and sweating relative to the unaffected side; edema and altered patterns of hair, skin, or nail growth in the affected region; reduced strength; tremors; and dystonia. The dramatic nature of its presentation, limited understanding of its mechanisms, and frequent lack of response to intervention has led to clinical confusion and misunderstanding in the past.