
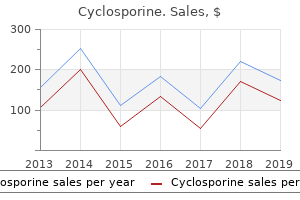
"Cheap cyclosporine online amex, symptoms uterine fibroids".
By: G. Karmok, M.A., M.D., M.P.H.
Co-Director, Howard University College of Medicine
Date physical therapy services began was 10-07-2019 treatment zit buy discount cyclosporine on-line, and dashes were used as the therapy end date value because the therapy was ongoing medications with weight loss side effect buy cyclosporine uk. Respiratory therapy services that were provided over the 7-day look-back period: · Respiratory therapy services; Sunday-Thursday for 10 minutes each day symptoms week by week purchase cyclosporine 25mg free shipping. Although a total of 50 minutes of respiratory therapy services were provided over the 7-day look-back period symptoms 12 dpo purchase cyclosporine discount, there were not any days that respiratory therapy was provided for 15 minutes or more. Rationale: There were no minutes or days of psychological therapy services provided over the 7-day look-back period. Recreational therapy services that were provided over the 7-day look-back period: · Recreational therapy services; Tuesday, Wednesday, and Friday for 30-minute sessions each day. Sessions provided were longer than 15 minutes each day, therefore each day recreational therapy was performed can be counted. Coding Instructions: Enter the number of calendar days that the resident received Speech-Language Pathology and Audiology Services, Occupational Therapy, or Physical Therapy for at least 15 minutes in the past 7 days. If a resident receives more than one therapy discipline on a given calendar day, this may only count for one calendar day for purposes of coding Item O0420. T also received 45 minutes of occupational therapy on Monday, Tuesday and Friday during the 7-day look-back period. T during the 7-day look-back period, item O0420 would be coded as 4 because therapy services were provided for at least 15 minutes on 4 distinct calendar days during the 7-day look-back period. F also received 90 minutes of occupational therapy on Monday, Wednesday and Friday during the 7-day look-back period. F received 60 minutes of speech-language pathology services on Monday and Friday during the 7-day look-back period. F during the 7-day look-back period, item O0420 would be coded as 3 because therapy services were provided for at least 15 minutes on 3 distinct calendar days during the 7-day lookback period. If the combined amount of group and concurrent therapy provided, by discipline, exceeds 25 percent, then this would be deemed as non-compliance and a warning message would be received on the Final Validation Report. Providers should follow the steps outlined below for calculating compliance with the concurrent/group therapy limit: · Step 1: Total Therapy Minutes, by discipline (O0425X1 + O0425X2 + O0425X3) · Step 2: Total Concurrent and Group Therapy Minutes, by discipline (O0425X2+O0425X3) · Step 3: Concurrent/Group Ratio (Step 2 result/Step 1 result) · Step 4: If Step 3 result is greater than 0. Coding Instructions for Speech-Language Pathology and Audiology Services and Occupational and Physical Therapies · Individual minutes-Enter the total number of minutes of therapy that were provided on an individual basis during the entire Part A stay. Concurrent therapy is defined as the treatment of 2 residents at the same time, when the residents are not performing the same or similar activities, regardless of payer source, both of whom must be in line-of-sight of the treating therapist or assistant for Medicare Part A. When a Part A resident receives therapy that meets this definition, it is defined as concurrent therapy for the Part A resident regardless of the payer source for the second resident. If the total number of minutes (individual plus concurrent plus group) during the stay is 0, skip this item and leave blank. Occupational Therapy Days-Enter the number of days occupational therapy services were provided over the entire Part A stay. A day of therapy is defined as skilled treatment for 15 minutes or more during the day. For example, if the resident received 20 minutes of concurrent therapy, the day requirement is considered met. Coding Tips and Special Populations · For detailed descriptions of how to code minutes of therapy and explanation of skilled versus nonskilled therapy services, co-treatment, therapy aides and students, please refer to these topic headings in the discussion of item O0400 above. Modes of Therapy A resident may receive therapy via different modes during the same day or even treatment session. The therapist and assistant should document the reason a specific mode of therapy was chosen as well as anticipated goals for that mode of therapy. Individual Therapy For a detailed definition and example of individual therapy, please refer to the discussion of item O0400 above. Therapy Modalities For a detailed definition and explanation of therapy modalities, please refer to the discussion of item O0400 above. While in the hospital, she exhibited some short-term memory difficulties specifically affecting orientation. Rationale: Individual minutes (including 53 co-treatment minutes) totaled 413 over the stay [(30 Ч 12) + 53 = 413]; concurrent minutes totaled 0 over the stay (0 Ч 0 = 0); and group minutes totaled 200 over the stay (20 Ч 10 = 200). Coding: O0425C1 would be coded 632, O0425C2 would be coded 200, O0425C3 would be coded 180, O0425C4 would be coded 47, O0425C5 would be coded 13. If a resident receives more than one therapy discipline on a given calendar day, this may only count for one calendar day for purposes of coding item O0430. T during the stay, item O0430 would be coded as 12 because therapy services were provided for at least 15 minutes on 12 distinct calendar days during the stay.
Adakveo is a first-in-class targeted monoclonal antibody that binds to P-selectin medicine upset stomach order discount cyclosporine on-line. All select pipeline assets are either investigational or being studied for (a) new use(s) medicine 773 buy generic cyclosporine 25 mg online. There is no guarantee that they will become commercially available for the use(s) under investigation symptoms after flu shot generic cyclosporine 25 mg online. Must meet the definition of treatment failure per the 2013 European Leukemia Net guidelines treatment 3 degree heart block order genuine cyclosporine on line. Cost-effectiveness of Evolocumab Therapy for Reducing Cardiovascular Events in Patients With Atherosclerotic Cardiovascular Disease (2017). As part of our longstanding commitment to improve health in Africa, we have entered into broad publicprivate partnership with Ghana government to tackle sickle cell disease, including access to available medicine, clinical research & use of digital technologies to achieve global standards of care. People with arthritis can find strength in each other, manage stress and take control of their health care through informed choices. Last year we began to elevate the level of patient involvement in the creation of Arthritis by the Numbers. We believe patients must be fully integrated into everything we do, and that their diverse needs and outcomes, the ones that are most important to them, are represented. We continue to grow that involvement in this third edition of Arthritis by the Numbers by adding: ·New sections and updating older sections, while trying to find answers to questions that were important to patients ·Facts from the "Osteoarthritis Voice of the Patient" report and the "Lupus: Patient Voices" report, as well as Arthritis Foundation survey data collected from arthritis patients ·Patient reviewer stories, telling us how arthritis. The 2019 edition of Arthritis by the Numbers includes three new sections and about 200 new and/or updated observations about arthritis. It can be used by a wide audience as a trustworthy set of verified facts, meant to inform patients and patient advocacy thought-leaders, elected officials, academics, drug/device industry professionals, rheumatology health care providers, researchers and many others. By prioritizing policies that further advance the needs of people with arthritis, we can accelerate the science of finding better treatments and cures. We invite you to get started with us by flipping through the 2019 Arthritis by the Numbers. Actually, "arthritis" is not a single disease; it is an informal way of referring to joint pain or joint disease. There are more than 100 different types of arthritis (see Appendix 1) and related conditions. People of all ages, genders and races can and do have arthritis, and it is the leading cause of disability in the United States. Conservative estimates only include patients who report they have doctor-diagnosed arthritis, indicating that more than 54 million adults and almost 300,000 children have arthritis or another type of rheumatic disease. A recent study attempted to include patients who were doctor-diagnosed with arthritis, as well as people who reported joint symptoms consistent with a diagnosis of arthritis. These adjusted estimates indicate there are potentially more than 91 million adults in the U. Another way of saying it: On the "ground floor" today, at least 54 million Americans suffer from arthritis; but the current "ceiling" may be almost twice that number. While researchers try to find more accurate ways to estimate the prevalence of this disease and the burdens it causes, we do know that it is most common among women, and the number of people of all ages with arthritis is increasing. They may stay about the same for years and then may progress or get worse over time. Severe arthritis can result in chronic pain, inability to do daily activities and make it difficult to walk or climb stairs. These changes may be visible, such as knobby finger joints, but often the damage can only be seen by X-ray. Some types of arthritis also affect other body parts, like the heart, eyes, lungs, kidneys and skin. The following facts describe some of the features common to many forms of arthritis. Those with obesity and arthritis are more likely to: - Have arthritis activity and work limitations - Be physically inactive - Report depression and anxiety - Have an increased risk of expensive knee replacement (Barbour 2016) - the prevalence of severe joint pain among adults with arthritis was stable from 2002 to 2014, but the absolute number of adults with severe joint pain was significantly higher in 2014 (14. An increase in obesity prevalence also occurred among those who reported meeting physical activity recommendations, those with very good/excellent health and those without heart disease, diabetes or serious psychological distress.
These cases signs: 44% were compared to a comparison group with a score of 2 or less medicine daughter lyrics 25mg cyclosporine for sale. Exposure: Ergonomic assessment measuring angles and distances of each operator seated at his/her workstation performed; Questionnaire responses to: Time spent in current job medicine checker buy cyclosporine 25 mg visa, time spent altogether keying or typing work symptoms 5 days after iui safe cyclosporine 25mg, training in the adjustment of their chair medicine that makes you throw up generic cyclosporine 25 mg visa, desk, or keyboard. Psychosocial and work environment scales included pertaining to job satisfaction as well as the Work Environment Scale [R. Outcome and exposure Outcome: Postal questionnaire on neck or shoulder symptoms frequency in last year, and influence on work methods, daily duties and activities or leisure time hobbies. For logistic regression model 12 month prevalence of neck and shoulder symptoms on 8 days or more. Exposure: Exposure based on occupation: Machine operators known to be exposed to static loading due to prolonged sitting and low-frequency whole body vibration, fast work pace, and upper trunk twisting. Carpenters exposed to dynamic physical work with varying postures and loads, static loading of neck/shoulder-arm, and male office workers, of whom only 40% were performing routine office tasks. Education, general health, and leisure time activities, car driving included in analysis. Daily symptoms: Daily symptoms: machine operators: 11% office carpenters: 8% workers: 2% Change work methods: machine operators: 19% carpenters: 21% Change work Machine vs. Outcome and exposure Outcome: Neck or shoulder complaints defined by questionnaire: Recurrent pain or aching in present work (during or after work). Exposure: Observation and interview; hr continuously sitting, standing time, survey of work postures, length of work cycle. Sewing machine operators found to have significantly greater static work compared to seamstresses. Subjects were part of a longitudinal study population that started in Finland in 1955; and from 1961 to 1963. The proportions of the highest income levels in the sample exceeded the Finnish population. Outcome and exposure Outcome: Based on Questionnaire data: Ache, pain, stiffness, numbness in their neck/shoulder in last 12 months. Severe neck disability: Pain for >7 days in last 12 months and mean disability index $ 15. Data collection in 1955 to 1963: Intelligence, alexithymia, social confidence, hobbies, motor development, verbal development, level of education of parents, type of income of family. Data collection in 1985: Questionnaire on family relationships, socioeconomic status, work history, characteristics of present work, job satisfaction, mental resources. Data collection in 1986 to 1987: Questionnaire: Physical characteristics of work, amount of physical exercise, illnesses, trauma. Measurements taken in adolescence, such as intelligence, alexithymia, social confidence, hobbies and socioeconomic status of the family showed no consistent association with neck/shoulder symptoms in adulthood. Only three studies specifically address the health outcome of shoulder tendinitis and these studies involve combined exposure to repetition with awkward shoulder postures or static shoulder loads. The evidence for specific shoulder postures is strongest where there is combined exposure to several physical factors like holding a tool while working overhead. The association was positive and consistent in the six studies that used diagnosed cases of shoulder tendinitis, or a constellation of symptoms and physical findings consistent with tendinitis, as the health outcome. Hagberg and Wegman [1987] attributed a majority of shoulder problems occurring in a variety of occupations to workplace exposure. Kuorinka and Forcier [1995] looked specifically at shoulder tendinitis and stated that the epidemiologic literature is "most convincing" regarding work-relatedness, especially showing an increased risk for overhead and repetitive work. The focus of this review is to assess evidence for a relationship between shoulder tendinitis and workplace exposures to the following: awkward postures, forceful exertions, repetitive exertions, and segmental vibration. Also included are studies relevant to shoulder disorders-as defined by a combination of symptoms and physical examination findings or by symptoms alone, but not specifically defined as tendinitis-and those studies for which 3-1 the health outcome combined neck and shoulder disorders, but where the exposure was likely to have been specific to the shoulder. Chapter 2 discusses studies involving neckshoulder disorders where assessment of exposure was likely specific to the neck region. The discussion within each risk factor is organized according to criteria presented on Pages 1-1 to 1-10 of the Introduction. Studies usually defined repetition, or repetitive work, for the shoulder as work activities that involved cyclical flexion, extension, abduction, or rotation of the shoulder joint. Repetitiveness was defined in four different ways in the reviewed studies: (1) the observed frequency of movements past pre-defined angles of shoulder flexion or abduction, (2) the number of pieces handled per time unit, (3) short cycle time/repeated tasks within cycle, and (4) a descriptive characterization of repetitive work or repetitive arm movements. Therefore, repetitive work should not be 3-2 considered the primary exposure factor, particularly independent of posture.
Using the arc system and its pointer medications xerostomia 25 mg cyclosporine, three or four points on the scalp are marked at specific values of 0 medicine of the future cheap 25 mg cyclosporine free shipping, [3 medications requiring prior authorization buy cyclosporine 25mg low cost, 7 treatment 4 stomach virus cheap 25mg cyclosporine with mastercard, A, and depth, Choose "easy" numbers for the angles, since the only constraint is that the points be distributed. The three or four marked scalp points are then confirmed to be at the same values of cz, [3, "/, A, and depth, thus establishing that the head ring has not moved. The target simulator contains a section of head ring that attaches to the top of the phantom base ring. The vertical coordinate must:be adjusted for the radius of the spherical target and for the thickness of the head ring, which should now overlay the phantom-simulated head ring. At the time of treatment, after the patient has been secured in the treatment position, these same three distances can be measured reasonably accurately (maybe:t 6 mm) on the patient using the lateral and ceiling lasers and a couple of rulers. Successful complelion of this test, even with its limited accuracy, can be very reassuring. Elements of a couch mount include: · Couch locking devices-Stabilize the couch to ensure mechanical stability and to disable all motions, · Lasers-Provide room-based fixed reference, · Patient docking device-Rigidly attaches to the couch and allows the patients frame to be uniquely positioned on the couch. Couch motions, except d e vertical movement, are locked and stabilizers applied if needed. This pro= cedure thus documents the alignment of the target with is*center through the film test and that the target coordinate is indeed the correct coordinate through the redundant entry on both devices. In practice, the lasers never are truly parallel even though they cross al the is*center, and small deviations will exist. Thus the critical eement is not that the lasers are perfectly collinear; instead the critical element is that they are stable from the time the treatment procedure starts until the treatment is over. Patient Alignment the following procedure is specific to the Radionics couch mount assembly and reflects the quality assurance procedure as performed at the Joint Center for Radiation Therapy (Tsai et al. A dynamic stereolaetic radiosurgical procedure starts with the couch at +75 ° and the gantry at 30% as shown in part (A). During the treatment the couch rotates 150° from +75* to -75 °, while the gantry simultaneously rotates from 30 ° to 330*. Several successive positions through which the couch and gantry move during the complete radiosurgical procedure are shown, starting (A) with the gantry and couch angels of 30* and 75°, respectively, through (B) 90* and +45°. Radiosurgery of cerebral arteriovenous malformations with the dynamic stere*tactic irradiation. Alignment Verification of a Couch-Mounted Frame (McGill) I the collimator alignment is a cddeal step in treatment because the precision of the treatment itself depends heavily on the accuracy of the collimafor placement. The collimator is placed onto the lianc tray holder, which is attached to the linac head. The proper collimator position is obtained with thehelpofceiling-and wall-mountedasersthatareperiodically l calibrated to indicate accurately the linac isocenter location. The alignment procedure is as follows: the couch table top is raised to the isocenter and the gantry positioned off-vertical, so that the dot produced by the vertical ceiling laser tO indicate the couch rotation axis is clearly visible on the table top. The position of the dot is marked on the table top, the gantry is placed vertically, and the collimator position is centered with the help of the light-field localizer lamp around the mark on the table top representing the couch rotation axis. The alignment of the collimator is verified with radiographic film in three steps. First, a film is suspended horizontally at the isocenter and exposed to a parallel-opposed beam with the gantry at 0 ° and 180". Next, another film is placed vertically through the isocenter and exposed to a parallel-opposed beam with the gantry at 90 ° and 270 °. Finally, a third film is placed horizontally through the isocenter onto the couch table top mid rotated with the couch during irradiation with a vertical beam. With the three-step process above, any misalignment of the collimator can be easily detected with the radiographic film. The radiosurgical treatment is not given unless the resalts of the alignment procedure are within the accepted tolerances. An example of the radiographic films obtained during an alignment proeedure for a l-cm diameter collimator is given in Figures 12 and 13. Part (a) of both figures represents the radiographic image of a single, vertical l-cm diameter beam.
Buy cyclosporine 25 mg line. New Way to Look for HIV.